
Treatment of the leaking mitral valve

Amongst physicians there is clear consensus that degenerative mitral valve disease (ruptured or stretched chords) is best treated with surgical repair. In other words, mitral valve repair is the gold standard treatment of degenerative mitral valve disease. This repair entails open heart surgery with assistance of the heart-lung machine (cardiopulmonary bypass). Mitral valve repair operations are not performed commonly by cardiac surgeons with less than 10 such operations performed by the average cardiac surgeon per year. Mitral valve operations, whether repair or replacements, can be performed via a median sternotomy (splitting of the sternum) or sternal-sparing techniques throughout the right chest. The sternal-sparing techniques can be divided into three:
Take Home Points:
Degenerative mitral valve disease (ruptured or stretched chords) is best treated with surgical repair
Experience counts, especially when it comes to mitral valve repairs.
Important questions to ask the surgeon:
How many mitral valve operations do you do in a year?
What is your repair rate?
How often do you perform minimally invasive valve mitral surgery?
1) Right minithoracotomy or keyhole approach (which is the most commonly used and with the most supporting medical data) in general 2-4 inch incision with 2 accessory ports.
2) Right chest endoscopic technique with port access with 1/2 inch to 1 inch incisions with 2 accessory ports.
3) Robotic assisted operations with 1/2 inch to 2 inch incision plus 3-4 accessory ports.
The techniques encompassed in repairs are multiple and overall all work well, some with advantages over others. Although newer therapies have made it to the market their role is in patients who are in the higher spectrum of illness, that is those who are so sick from multiple causes that undergoing open-heart surgery becomes a high-risk endeavor.
It is well known and published that the higher the number of mitral valve repair operations performed by a surgeon, the higher the repair rate. In other words, experience counts, especially when it comes to mitral valve repairs. This is even more important when it comes to minimally invasive mitral valve repairs and complex mitral problems, as these operations have a very steep learning curve. Important questions to ask the surgeon: how many mitral valve operations he or she does in a year, what the repair rates are, and how often he or she performs minimally invasive valve operations.
Mitral valve repair in current times should be performed by surgeons with experience performing specifically simple to complex mitral valve repairs. It should also be performed in centers of excellences where the care is geared towards having the best possible outcome after surgery. The American Heart Association and American College of Cardiology Guidelines recommends that these centers have excellent outcomes with low risk for mortality or complications. The minimally invasive approach should not be an added value, but the standard of care for mitral valve surgery.
For persons who are either frail, too ill to undergo surgery, or have a true contraindication to open heart surgery of any kind there is an alternative therapy that is also least invasive called the mitral clipping. This is performed via a vein in the groin and is performed by both cardiologists and surgeons under general anesthesia, but without the heart lung machine. The goal of this therapy is to diminish the severity of the mitral leakage and therefore improve symptoms and in some cases prolong life.
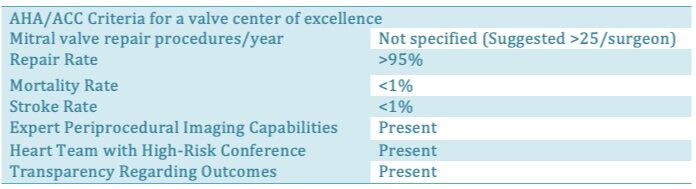
This table summarizes the American Heart Association and American College of Cardiology as well as Society of Thoracic Surgeons recommendations for mitral valve repair in cases of patients with severe mitral leakage.
Who should perform my mitral valve operation?

In an article by Gammie published in 2009 the landscape of mitral valve surgery in the United States over a period of 4 years was studied. The authors looked at what percentage of mitral valve operations performed were repairs versus replacements. They found that the number of patients undergoing repairs had increased in an 8-year period from 51 to 69% for patients with leaky valves. They did find that the mortality or chances of death after mitral valve replacement were higher than after mitral valve repair (3.8% versus 1.4%). In the healthiest of patients undergoing mitral valve repair (what we call asymptomatic patients) the risk of death was 0.6%. In the same 8-year time period more biological man-made valves were implanted with a decrease rate of mechanical valve implantation from 68% to 37%. (Gammie, James S., et al. "Trends in mitral valve surgery in the United States: results from the Society of Thoracic Surgeons Adult Cardiac Database." The Annals of thoracic surgery 87.5 (2009): 1431-1439.)
In 2018 Gammie and coauthors again published a landmark article in which they described the current state of mitral valve surgery in the United States. The focus this time was on degenerative disease (ruptured or stretched chords). What they found was a total increase in mitral valve surgery performed in the country with an increase of 24% for a total of 87,214 operations in 1,125 centers. This number would assign 77.5 valves operated per center! Most centers have three or more surgeons. They further shed light on the volume of mitral valve surgery performed by the average cardiac surgeon. The rate of mitral valve repair had decreased from 67% to 63% in three years. The repairs consisted of 46% leaflet resection and 23% artificial chordal implantation.
“Less invasive operations were performed in only 23% of all mitral valve cases. ”
Less invasive operations were performed in only 23% of all mitral valve cases. Importantly 16% of all valve replacements performed had an attempt at repair before replacing the valve.

A right minithoracotomy incision for a minimally invasive mitral valve operation.
In all, what we can conclude from these two important studies is that repair of the mitral valve carries an advantage in survival to replacement; yet the repair rate is only 63% nationwide for degenerative disease (ruptured or stretched chords) when it should be closer to 90%. The number of valves replaced after an attempted repair in a 5-year period was very large (4,855 of 29,970 or 16%). This data is contemporary (2011-2016).
“The repair rate is only 63% nationwide for degenerative disease ”
The importance of all this is that there is a clear deficit in the knowledge and technical base among cardiac surgeons to repair the mitral valve. Moreover, these abilities are perhaps becoming scarcer as the number of repairs decreased.
The authors went a step further and looked at the volume of surgery for the mitral valve performed by different centers. In the country 106 centers performed ZERO mitral valve operations for degenerative disease. 763 centers performed 0-6 operations/year. 213 performed 6-25/year. 28 performed 25-50/year 11 performed 50-100/year Only 4 centers performed more than 100/year. (Gammie, James S., et al. "Isolated mitral valve surgery: The Society of Thoracic Surgeons adult cardiac surgery database analysis." The Annals of thoracic surgery 106.3 (2018): 716-727.)
“763 (out of 1125) centers performed zero mitral valve operations for degenerative disease.”
The answer to the question of who should perform your mitral valve operation is then easy to answer. A Center AND Surgeon that perform more than 50 such operations per year. The reason is simple, repetitions begets good results. This is only part of the answer to the question of who should perform my operation for the mitral valve. The next necessary question is which one of these centers/surgeons has achieved a high degree of good outcomes by objective criteria, not by word of mouth. This point is so important that the American Heart Association and American College of Cardiology and the Society of Thoracic Surgeons have incorporated this in the formal recommendations (Nishimura, Rick A., et al. "2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines." Journal of the American College of Cardiology 70.2 (2017): 252-289.).
Guidelines recommend that asymptomatic patients with severe mitral leakage be operated on in centers, and by surgeons with a 95% likelihood of durable successful repair and with less than 1% chance of death. The Society of Thoracic Surgeons (STS) created many decades ago a National Database where all outcomes of cardiac surgeons are recorded including the risk profile for any particular person. The STS awards a 3 star rating to centers that achieve the highest level of quality care. This is not a physician popularity peer to peer vote. The STS uses objective data and compares the outcomes of any surgeon or center to that of others nationwide. This is indeed the most objective and comprehensive descriptor of cardiac surgery outcomes by center.
The landing page for the public reporting of the STS database is: https://publicreporting.sts.org The page for reporting by State is: https://publicreporting.sts.org/search/mvrr_report_card/hospital
“77% of cardiac surgeons perform mitral valve surgery via a median sternotomy”
The last part of the answer to the question of “who should perform my mitral valve operation” is how it is done. This is the approach. Seventy seven percent of surgeons perform isolated mitral valve surgery through a sternotomy or splitting the sternum. Although this approach is time tested and effective it does prolong recovery, is associated with more pain and more transfusions. The results of repairs performed minimally invasive are as durable as a sternotomy approach and many surgeons argue this should be the new standard of care. This last part is not easy to come by.
The information of who performs minimally invasive mitral surgery many times is distorted by healthcare systems for the sake of attracting patients. Often times healthcare systems will advertise robotic-assisted surgery when in reality it is not used to repair the mitral valve or the experience with this technology is very limited at that site. In other circumstances it is advertised as superior to all forms of mitral valve surgery which is not the truth. Others advertise a minimally invasive approach and the incision is, indeed, not a sternotomy (splitting of the sternum), but the length of the incision is such that it constitutes a thoracotomy or full incision on the right side, one that will be painful.
This website is an attempt to identify the surgeons and centers that perform high volume minimally invasive mitral valve surgery across the country with high quality markers.
In conclusion, a mitral valve operation should be performed at centers and by surgeons that have significant experience repairing and replacing valves and that can perform the operation minimally invasive.